
Sitting topless in the examining room at your plastic surgeon’s office planning breast augmentation surgery can be a very stressful experience for a woman.
Usually, the mind reels: “What will the surgeon think?” “I have never been topless in front of a stranger before?” “ I must be crazy for even being here.” “What if he laughs?” “What if we pick the wrong size implants?” And on and on the questions go.
I remember early in my career, seeing a young woman interested in breast augmentation surgery. After our initial conversation, I stepped out so she could change into a gown for the examination. When I came back in the room, out of sheer embarrassment, she simply could not remove her gown to allow the physical exam to proceed. This was the case despite her real wish to have the surgery. She got dressed, left the office, and I never saw her again.
I learned a valuable lesson from that young lady. I have never forgotten her, and what she taught me about the stress and anxiety women can feel in a surgeon’s examining room.
But have you ever wondered exactly what the surgeon is thinking during the examination? It’s a fairly complex and regimented mental process. What follows is a peek inside my head during the physical examination part of a breast augmentation consultation.
Is there symmetry?
The first quality I look at is symmetry. Or rather, the degree of asymmetry, since no two breasts are ever mirror images of each other. Which breast is bigger, and by how much? Do I need two different sized implants, or can I make up the difference with a bit of fat grafting? Or can the difference simply be ignored? Is one side of the rib cage more prominent than the other? Is the sternum (breastbone) sticking out or caved in? If so, is there some scoliosis (curvature of the spine) present causing the difference? Are the infra-mammary folds even? (I can tell immediately by the indentations left by your bra). What is the difference in nipple height, and forward projection of the breasts?
In almost every case, I will point out asymmetries the patient never noticed before. It’s critical that we discuss those, since some I can fix, and some I cannot.
What is the Skin quality?
The quality of the skin envelope of the breast is critical to planning a beautiful breast augmentation. Is the skin thick and full of elasticity? Is it thin and stretched out? Are there stretch marks? If so, where are they? How much volume is needed to “fill” the existing skin envelope? Will the skin be able to support the weight of the implant? Are there pre-existing scars from earlier surgery or trauma? Is there evidence of sun damage?
This part of the exam is critical, because while the skin can be tightened or trimmed or filled, it’s nature, as determined by your genetics, can’t be changed. We have to play the hand we are dealt.
Is there Ptosis?
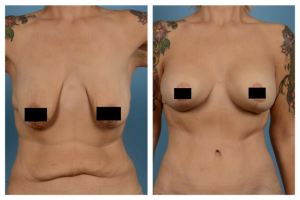
Example of a patient with ptosis who required a breast lift as well as implants.
Ptosis means how “droopy” the breasts are. Are the nipples pointing up, straight ahead, or down to the floor? If they need to be lifted, by how much, and what sort of incision pattern will I need? Maybe just a small circular incision around the areola? Maybe around the areola with the addition of a vertical skin removal?
This part of the examination is critical because many women think that the addition of an implant can fix the intended ptosis issue as well, which is almost never the case.
Nipple – Areola Complex.
How big is the areola? Will it “fit” the proportions of the new breast? Does the areola need to be reduced in diameter? Is there nipple inversion? If yes, how severe? On one side or both? Is the pigmented border of the areola sharply defined, or does the colour gradually fade? Is the nipple size and projection normal? Is it symmetrical?
What is the nature and distribution of the breast parenchyma?
All breasts are made up of a combination of glandular breast tissue and fat. What is the ratio? Is the breast mostly fat, mostly gland, or an even mix? What is the distribution of the parenchyma? Is the upper pole full, depleted or somewhere in the middle? Do I need to remove some of the heavy tissue along the bottom of the breast? Do I need to supplement the upper pole with an implant that will reach up there, or should I fill the upper pole with some soft, all-natural fat graft from the tummy or thighs?
This part of the examination is important because the nature of the parenchyma will determine the softness and “naturalness” of the final result. A nice thick, soft layer of gland and fat will always produce a more pleasing result than an augmentation done on someone with very little gland and fat.
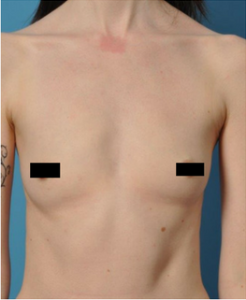
Example of a low breasted patient.
Are you a high or low breasted woman?
Some breasts sit high on the chest wall. Some sit lower. That is a feature that is essentially impossible to change. I need to note it because low breasted women always want to be high breasted and I can’t do it. That doesn’t mean they won’t have a spectacular result; it just means I can’t move the breasts from the middle of the chest to up under the collarbones.
What is the overall breast volume and base width?
How big is the breast now? Did you say you wore an A or B cup bra, but you actually have much more volume than that? Or the opposite? I never want the breast implant to make up the vast majority of the breast volume after surgery, so the volume before surgery is critical. Maybe you thought you “needed” a breast implant, but you have enough volume that a lift and some upper pole fat grafting would be ideal instead. What is the width of the base of the breast? I need to make sure that the implants we choose aren’t too wide so that they won’t end up in your armpit, or across your midline. Nobody likes that!
Can I meet your expectations?
By this time, we have already had a detailed discussion about your goals, and I have just about completed the physical exam. I should have a good idea by this point as to whether or not I can give you what you want and need. If I can, I will tell you so, and we will discuss the plan. If I can’t, I will tell you that too, and we will move on to plan B.
Are you sweating?
I bet you didn’t see this question coming. Sometimes patients will really sweat during the examination. It’s natural, and it doesn’t bother me at all, but it does tell me that you are feeling very anxious. When I see the sweat dripping from your armpits, I will take just a brief second reassure you that all is well, while at the same time I will take care to conduct the examination expeditiously so as not to prolong the agony for you.
So there you have it. That’s what is going on in my head while I do the physical examination for a breast augmentation procedure. Each step is critical if the best possible result is expected. While it seems like a lot to do, it actually only takes a few short minutes. At least it should, if the surgeon you are seeing is experienced, and well trained.
